
What's the relationship between the hip and the pelvic floor?
Why a question about your bladder/bowel/sexual health is important during your hip check up?


Are you someone who started experiencing pain with intercourse after getting diagnosed with a labral tear?
Or feel a deep pain in the groin after every run that you can’t tell if it’s coming from your hip or the pelvic floor?
And what about the deep buttock pain? Is it your piriformis (hip muscle) or coccygeus (pelvic floor muscle) that sits right next to the piriformis?
What is this mystery here? And what is the connection between the pelvis and the hip?
Well, we all know that the pelvis and hips sit next to each other in our bodies; so, it shouldn’t be a huge surprise that they impact each other in some manner (in fact, the hip bone femur connects to the pelvis to form the hip joint). Even though we can see that these two regions are connected, most healthcare providers do not ask questions about pelvic health when a patient walks in with a complaint of hip pain or vice versa.
Understanding how exactly the hip and pelvis support each other and which anatomical structures they share can really help assess a variety of pelvic conditions, ranging from pelvic floor dysfunction to urinary urgency and frequency, and from dyspareunia (painful sex) to even constipation. Unfortunately, if this assessment isn’t done thoroughly, the root cause can be easily missed and the problem can eventually turn chronic. 😥
So, let’s learn about some of the structures that are shared by these two neighbors:
MUSCLES:
Most hip muscles connect to at least some part of the pelvis. So, pelvic movement/mobility can definitely affect the length-tension relationship of these muscles. For example, all the adductor muscles connect to the inferior pubic ramus and ischial ramus (both are a part of the pelvis). But let’s look at two specific muscles that lie very close to the pelvic floor muscles and can affect their function:
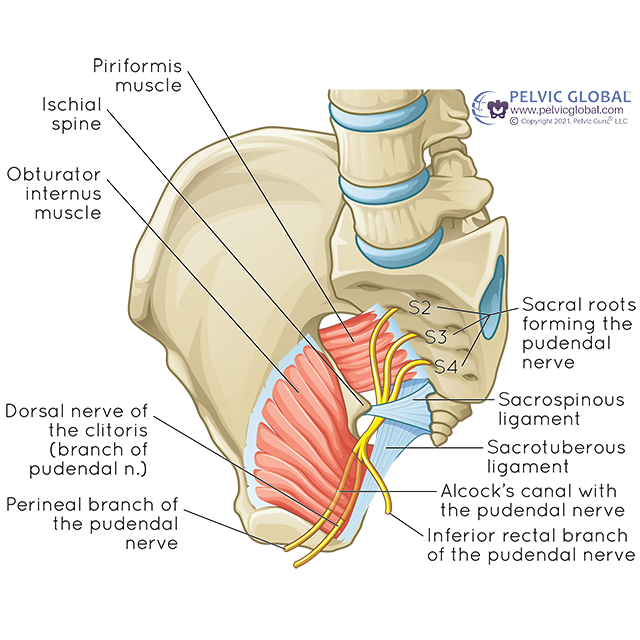
Obturator internus (OI): a deep stabilizer of the hip joint; it is also considered a part of the pelvic floor and forms its sidewalls. OI is an external rotator of the hip and its fascia produces a sheath that forms Alcock’s Canal in the pelvis, through which the pudendal nerve, artery, and vein pass through, after crossing the ischial spine. OI can be confused with hip labral pain and can create symptoms of urinary urgency/frequency. Alcock’s canal is one of the common areas where the pudendal nerve can get entrapped and cause issues such as burning, and stabbing pelvic pain.

Piriformis: a deep hip stabilizer that also rotates the hip externally. It isn’t considered a part of the pelvic floor but sits right next to the Coccygeus muscle in the pelvic outlet. When overactive/tense, it can cause deep buttock pain and can also trap the pudendal nerve. Compression of the pudendal nerve can then create overactivity in the pelvic floor muscles along with burning and stabbing pelvic pain.
Hypermobility of the hip joint: Pelvic floor dysfunction is quite commonly seen in people with hypermobility of the hip joint. Due to either weakness in the hip musculature or a lack of stability of the joint itself, pelvic floor muscles often end up taking up the slack of its not-so-strong neighbor. This additional work of providing stability to the hip joint, therefore, sometimes leads to pelvic floor dysfunction.
NERVES:
The pelvic region is richly supplied by a web of nerves owing to its multiple life-sustaining functions. The nerves ilioinguinal, genitofemoral, and posterior cutaneous femoral nerve provide an overlapping supply to both the hip and the pelvic region, such as the groin, inner thigh, external genitals, and the perineum region, which could be easily confused with the pudendal nerve, and therefore, often times gets misdiagnosed.
Genitofemoral Nerve: primarily a sensory nerve that arises from the L1 and L2 nerve roots of the spinal cord:
Provides sensation to:
Upper thigh region
Front of the scrotum
Mons pubis and outer labia
Provides motor function to:
The Cremaster muscle and helps retract the testes and is responsible for the ‘Cremaster Reflex’
Ilioinguinal nerve: primarily a sensory nerve that arises from the T12 and L1 nerve roots of the spinal cord:
Provides sensation to:
Pubic symphysis
The top inner part of the thigh
Outer labia
The root of the penis and the front of the scrotum
Provides motor function to:
Trasnverse abdominis and Internal oblique muscles (in the abdomen)
Posterior Cutaneous Femoral nerve: primarily a sensory nerve that arises from the sacral plexus with nerve roots S1-3. Different branches provide sensations to different areas:
Provides sensation to:
Inferior cluneal nerve: outer and lower parts of the buttock
Perineal branch: supplies the back of the outer labia and the scrotum
Cutaneous branch: supplies the skin of the back of the thigh, inside of the thigh all the way to the popliteal fossa (back of the knee).
Pudendal Nerve: is a mixed nerve with both sensory (provides sensation) and motor function (supplies muscles). It arises from the sacral nerve roots (S2, S3, S4) of the spinal cord.
Provides sensation to:
Perineal skin
Inner & outer labia, back of the scrotum
clitoris and penis
Provides motor function to:
Pelvic floor muscles
Urethral Sphincter
External anal sphincter
And thus helps us stay continent
LIGAMENTS:
Sacrotuberous Ligament: originates from the sacroiliac (SI) joint capsule, sacrum, and coccyx and attaches to the ischial tuberosity (sit bone), where it blends with the fibers of the biceps femoris Tendon (part of the hamstring muscle) and provides an extensive base for the gluteus max insertion. Any change in the mechanics of the pelvis can create tension in these muscles (or vice versa), commonly resulting in pain with sitting.
Sacrospinous Ligament: connects the sacrum to the ischial spine in the pelvis and creates the greater sciatic notch through which the sciatic nerve passes. Should be carefully differentiated from the pudendal nerve.
The pudendal nerve passes in between these two ligaments near the ischial spine, which is one of the most common sites for the entrapment of the nerve. Entrapment of the pudendal nerve at this level can cause pain all the way from the anus to the clitoris/ tip of the penis. All pudendal neuralgia is not caused by entrapment of the nerve and should be carefully examined for the appropriate medical treatment.
So, as you can see these regions share more than just a handful of structures and need to be in total harmony in order to support one another.
It might sound weird, at first, when your healthcare provider asks questions about bladder, bowel, or sexual history during an exam for your hip pain. But I now hope that you have a better understanding of how intricately these two systems are interconnected 🔗.
References:
Ali A, Andrzejowski P, Kanakaris NK, Giannoudis PV. Pelvic Girdle Pain, “Hypermobility Spectrum Disorder and Hypermobility-Type Ehlers-Danlos Syndrome: A Narrative Literature Review.” J Clin Med. 2020 Dec 9;9(12):3992. doi: 10.3390/jcm9123992. PMID: 33317183; PMCID: PMC7764306.
Kaur J, Leslie SW, Singh P. “Pudendal Nerve Entrapment Syndrome.” [Updated 2022 Nov 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544272/
Chaudhry SR, Imonugo O, Jozsa F, et al. “Anatomy, Abdomen and Pelvis, Ligaments.” [Updated 2022 Nov 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK493215/